-
14
-
Alex Jones Was Right wrote:
Your links are dogsh!t
23 -
Thread has gone full blown schizophrenic
32 -
Congratulations to Pfizer. The "vaccine" sales are on a downward slope, but they milked it for all it was worth. Indemnification is a license to operate the profit train at maximum speed.
22 -
DanM wrote:
Congratulations to Pfizer. The "vaccine" sales are on a downward slope, but they milked it for all it was worth. Indemnification is a license to operate the profit train at maximum speed.
Pfizer sales are down after everyone took the shots they felt they needed? This is revelatory how? You’re grasping at straws here Dan.
34 -
Alex Jones Was Right wrote:
I dont care if you’re vaccinated or not. I just find it odd at the amount of time you spend searching the internet for vaccine injuries. It’s quite sick and a disturbing personality trait tbh
23 -
Lonely existence for the anti vaxxers here. I wish you well.
24 -
DanM wrote:
Congratulations to Pfizer. The "vaccine" sales are on a downward slope, but they milked it for all it was worth. Indemnification is a license to operate the profit train at maximum speed.
It would seem an awful lot of people have awakened and are done with these boosters.
32 -
Newname wrote:
DanM wrote:
Congratulations to Pfizer. The "vaccine" sales are on a downward slope, but they milked it for all it was worth. Indemnification is a license to operate the profit train at maximum speed.
It would seem an awful lot of people have awakened and are done with these boosters.
I took two boosters and I’m probably good to go. I’ll see what emerging evidence comes out. I kind of follow Paul Offit who has been critical of boosters for young people. Please note he is very much for the vaccine. See how balanced and nuanced I am? It’s almost like I’m not an ideologue.
23 -
It’s highly likely that the boosters (3rd plus dose) are inducing B cell memory class switching to the immune tolerant IgG4 antibodies, with the inability to cultivate sterilizing infection, which might explain the negative efficacy witnessed in some patients, as well as the stronger virulence of otherwise fairly innocuous Omicron kin. We don’t know. But it needs to be pursued further before we just go giving annual mRNA “boosters.” Note that natural infection doesn’t elicit the same class switching.
https://www.science.org/doi/10.1126/sciimmunol.ade2798
“In the present study, we longitudinally tracked the antibody response in volunteers vaccinated with two or three doses of Comirnaty for a period of at least 8 months after the first vaccination. We found an mRNA vaccine–driven expansion of memory B cells expressing IgG4. We detected spike-specific IgG4 antibodies in about half of the serum samples collected 5 to 7 months after the second immunization, all of which did not show any IgG4 at earlier time points. For all other IgG subclasses, a decline was seen in the same period. Moreover, after the third immunization, IgG4 levels sharply increased and became detectable in almost all vaccinees.
In line with the proposed ongoing GC reaction, the appearance of IgG4 antibodies might be a consequence of consecutive events of CSR and the maturation of IgG4-switched memory B cells. IgG3 antibodies were less efficiently boosted and did not reach the levels seen after the second dose. Considering the order of the four γ heavy-chain genes (γ3-γ1-γ2-γ4) within the immunoglobulin gene complex on chromosome 14 (21), this would support the hypothesis of consecutive CSR from proximal IgG3 to distal IgG4 (28, 33). It is reported for the adult immune repertoire that CSR toward IgG2 or IgG4 is more frequently occurring from IgG1 B cells than from IgM/IgD cells (33).
When we isolated spike-specific memory B cells from vaccinees 210 days after the second vaccination and 10 days and 5 months after the third vaccination, we confirmed by flow cytometry and single-cell sequencing the presence of substantial numbers of spike-reactive, IgG4-switched B cells, whereas IgG3-positive clones were hardly detectable. We cannot formally rule out de novo class switching toward IgG4 immediately after booster vaccination. However, the presence of IgG4 antibodies in the sera at that time point, together with the rapid rise of IgG anti-spike serum antibodies, supports the idea of a reactivation of already present IgG4 memory B cells through the booster immunization.
In a cohort of breakthrough infections, the anamnestic IgG4 antibody response correlated with the time interval between immunization and infection. Individuals who experienced a breakthrough infection within the first 70 days after the second vaccination did not have substantial serum levels of anti-spike IgG4 at their first visit, which also did not significantly increase during the following observation period. In contrast, anamnestic IgG4 responses were seen when breakthrough infections occurred later than 3 months after the second immunization and were robustly detectable when the study participants had been vaccinated three times before infection. Although the number of individuals studied was limited, and we did not stratify for potential confounding factors (e.g., the initial viral load, severity of disease, or the VOC causing the infection), the presented data are consistent with the hypothesis of a slowly developing pool of IgG4-switched memory B cells after two doses of mRNA vaccines. Furthermore, we observed significantly higher IgG4 levels after two doses of Comirnaty mRNA vaccine compared with a heterologous immunization regimen with a primary Vaxzevria vaccination followed by one dose of Comirnaty, although the total anti-spike IgG response was comparable. This argues against the hypothesis that repeated exposure to the spike protein itself triggers the unusual IgG4 response. It is currently not clear whether or to what extent the Comirnaty mRNA vaccination or the short interval of immunizations is responsible for the observed long-lasting GC reactions (12–14), but a prolonged presence of vaccine mRNA or antigen in the lymph node might be a potential explanation (12). Furthermore, a robust and persistent T follicular helper (TFH) cell response for up to 6 months after mRNA vaccination has been described in draining lymph nodes (17), which might be involved in the regulation of CSR by recurrent interactions of GC B cells with TFH cells. Of note, our study was restricted to vaccinees receiving the Comirnaty vaccine. Because the quantities and the functional profile of spike-specific antibodies induced by Comirnaty and mRNA-1273 have been reported to be slightly different (6, 34), it will be interesting to analyze whether repeated vaccination with mRNA-1273 induces a similar switch to noninflammatory IgG subclasses.Independent of the underlying mechanism, the induction of antiviral IgG4 antibodies is a phenomenon infrequently described and raises important questions about its functional consequences. Neutralizing antibodies preventing the initial binding of the viral particle to its specific cellular receptor are considered to be the most protective measure against SARS-CoV-2 infections (35). This competitive binding is mediated by the variable antigen-binding site and does not rely on the constant part of the Fc fragment. In the present study, we confirmed previous reports on improved avidity and neutralizing potential of vaccine-induced antibodies after the third vaccination (9–11). However, the large number of breakthrough infections caused by the Omicron variant indicates that current vaccination regimens do not confer sterilizing protection. Once infection is established, Fc-mediated effector functions become more relevant to clear viral infections. Systemic serology approaches have even revealed that different antibody functions can contribute to various degrees to protection dependent on the viral pathogen, as shown for influenza viruses, RSV, or SARS-CoV-2 (36–39). Passive immunization studies in animal models have further demonstrated that the degree of protection achieved by the application of mAbs depends on their IgG subclass (40–43). In this regard, IgG4 is considered an anti-inflammatory IgG with low potential to mediate Fc-dependent effector function such as ADCC or ADCP (20, 44).
High levels of antigen-specific IgG4 have been reported to correlate with successful allergen-specific immunotherapy by blocking IgE-mediated effects (45). In addition, increasing levels of bee venom–specific IgG4 have been detected in beekeepers over several beekeeping seasons and lastly even became the dominant IgG subclass for the specific antigen, i.e., phospholipase A (PLA). The IgG4 response is characterized by a very slow kinetics and takes several months to appear, whereas PLA-specific IgG1 antibodies were already measurable at earlier time points, which resembles our findings in this study (46). Furthermore, an increase in PLA-specific IgG4-switched B cells was observed in patients undergoing specific immunotherapies (SITs) (47).
So far, few studies on the role of vaccine-induced IgG4 responses against infectious diseases are available. In the field of HIV vaccine development, repeated protein immunization in the trial VAX003 (48) led to higher levels of HIV gp120-specific IgG2 and IgG4, whereas a prime-boost immunization with a canarypox vector (ALVAC-HIV) and the same protein vaccine in the RV144 trial (49) resulted in higher HIV-specific IgG3 responses correlating with partial protection against HIV (50, 51). Furthermore, the vaccine-elicited IgG3 antibodies enhanced effector functions as ADCC and ADCP, but vaccine-induced IgG4 inhibited those functions (51).With respect to the control of viral infections, little is known regarding virus-specific IgG4 antibody responses. As shown here for RSV-specific IgG responses, IgG4 is hardly induced by acute respiratory viral infections even after repeated exposure. Although measles-specific IgG4 antibodies can be induced by natural infection (52), even chronic viral infections such as human cytomegalovirus (HCMV) do not trigger significant specific IgG4 antibodies (53).
There are very few reports on the induction of IgG4 after natural infection with SARS-CoV-2. The dominant subclasses were mostly IgG1 and IgG3 (54–56).Nevertheless, a Brazilian study during the early phase of the pandemic correlated an early onset and high levels of anti-spike IgG4 antibodies with a more severe coronavirus disease 2019 (COVID-19) progression after SARS-CoV-2 infection, which might indicate a less effective antibody response (56). In addition, Della-Torre et al. (57) reported on a significant association of high IgG4/IgG1 ratios with poor disease outcome. However, in the case of a primary immune response, the causality is difficult to address because it is also possible that a more severe infection leads to an IgG4 response and not vice versa.
In our study, antibody-mediated phagocytic activity and complement deposition were reduced in sera after the third immunization, in parallel to higher proportions of anti-spike IgG4 antibodies. However, how these changes affect subsequent virus infections remains unclear. Because Fc-mediated effector function could be critical for viral clearance, an increase in IgG4 subclasses might result in longer viral persistence in case of infection. However, it is also conceivable that noninflammatory Fc-mediated effector functions reduce immunopathology, whereas virus is still being neutralized via high-avidity antibody variable regions. In a cohort of vaccinees with breakthrough infections, we did not obtain any evidence for an alteration of disease severity, which was mild in almost all of our cases. Larger cohorts with differential disease severities will be needed to address this aspect in the future. However, our results demonstrate that a subsequent infection can further boost IgG4 antibody levels, with IgG4 becoming the most dominant among all anti-spike IgG subclasses in some individuals.In summary, our study demonstrates an mRNA vaccine–induced antiviral IgG4 antibody response appearing late after secondary immunization. Further investigations are needed to clarify the precise immunological mechanisms driving this response and to evaluate whether an IgG4-driven antibody response affects subsequent viral infections and booster vaccinations. This is relevant not only for potential future vaccine campaigns against SARS-CoV-2 but also for new mRNA-based vaccine developments against other pathogens.”
23 -
DanM wrote:
The sick wildebeest that is the vax mob mafia keeps on turning around and around and around, scraping the bottom of their propaganda barrel.
Take a look at this poor soul. Indoctrinated to the point of delusion. Unable to grasp reality after multiple "vaccine" injections.
The cognitive dissonance is strong with this one.
21 -
Covidiocy wrote:
DanM wrote:
The sick wildebeest that is the vax mob mafia keeps on turning around and around and around, scraping the bottom of their propaganda barrel.
Take a look at this poor soul. Indoctrinated to the point of delusion. Unable to grasp reality after multiple "vaccine" injections.
The cognitive dissonance is strong with this one.
Read some of the comments in the NY Times today. The following is but one example.
"After 5 vaccinations I contracted COVID in November 2022. I’m 72 and many friends and relatives in the same age group and also vaccinated have contracted COVID in the last 6 months. When I tested positive I called my GP, she said drink lots of fluids. I developed a very sore throat making it difficult to swallow and breathe. After 4 days I called the doctor again and was prescribed prednisone which helped greatly. A couple of weeks later I developed heart problems, like other friends in my age group. This disease is not done yet, old people should be warned about the risks. Anti viral medication should be prescribed immediately."
02 -
Notice how anti vaxxers don’t engage with anyone who is pro vaccine. They are scared of actual debate with regular humans. This thread is done as far as I’m concerned.
32 -
DanM wrote:
Covidiocy wrote:
The cognitive dissonance is strong with this one.
Read some of the comments in the NY Times today. The following is but one example.
"After 5 vaccinations I contracted COVID in November 2022. I’m 72 and many friends and relatives in the same age group and also vaccinated have contracted COVID in the last 6 months. When I tested positive I called my GP, she said drink lots of fluids. I developed a very sore throat making it difficult to swallow and breathe. After 4 days I called the doctor again and was prescribed prednisone which helped greatly. A couple of weeks later I developed heart problems, like other friends in my age group. This disease is not done yet, old people should be warned about the risks. Anti viral medication should be prescribed immediately."
Person is citing the disease not the vaccine as a cause of complications
31 -
Covidiocy wrote:
It’s highly likely that the boosters (3rd plus dose) are inducing B cell memory class switching to the immune tolerant IgG4 antibodies, with the inability to cultivate sterilizing infection, which might explain the negative efficacy witnessed in some patients, as well as the stronger virulence of otherwise fairly innocuous Omicron kin. We don’t know. But it needs to be pursued further before we just go giving annual mRNA “boosters.” Note that natural infection doesn’t elicit the same class switching.
https://www.science.org/doi/10.1126/sciimmunol.ade2798
“In the present study, we longitudinally tracked the antibody response in volunteers vaccinated with two or three doses of Comirnaty for a period of at least 8 months after the first vaccination. We found an mRNA vaccine–driven expansion of memory B cells expressing IgG4. We detected spike-specific IgG4 antibodies in about half of the serum samples collected 5 to 7 months after the second immunization, all of which did not show any IgG4 at earlier time points. For all other IgG subclasses, a decline was seen in the same period. Moreover, after the third immunization, IgG4 levels sharply increased and became detectable in almost all vaccinees.
In line with the proposed ongoing GC reaction, the appearance of IgG4 antibodies might be a consequence of consecutive events of CSR and the maturation of IgG4-switched memory B cells. IgG3 antibodies were less efficiently boosted and did not reach the levels seen after the second dose. Considering the order of the four γ heavy-chain genes (γ3-γ1-γ2-γ4) within the immunoglobulin gene complex on chromosome 14 (21), this would support the hypothesis of consecutive CSR from proximal IgG3 to distal IgG4 (28, 33). It is reported for the adult immune repertoire that CSR toward IgG2 or IgG4 is more frequently occurring from IgG1 B cells than from IgM/IgD cells (33).
When we isolated spike-specific memory B cells from vaccinees 210 days after the second vaccination and 10 days and 5 months after the third vaccination, we confirmed by flow cytometry and single-cell sequencing the presence of substantial numbers of spike-reactive, IgG4-switched B cells, whereas IgG3-positive clones were hardly detectable. We cannot formally rule out de novo class switching toward IgG4 immediately after booster vaccination. However, the presence of IgG4 antibodies in the sera at that time point, together with the rapid rise of IgG anti-spike serum antibodies, supports the idea of a reactivation of already present IgG4 memory B cells through the booster immunization.
In a cohort of breakthrough infections, the anamnestic IgG4 antibody response correlated with the time interval between immunization and infection. Individuals who experienced a breakthrough infection within the first 70 days after the second vaccination did not have substantial serum levels of anti-spike IgG4 at their first visit, which also did not significantly increase during the following observation period. In contrast, anamnestic IgG4 responses were seen when breakthrough infections occurred later than 3 months after the second immunization and were robustly detectable when the study participants had been vaccinated three times before infection. Although the number of individuals studied was limited, and we did not stratify for potential confounding factors (e.g., the initial viral load, severity of disease, or the VOC causing the infection), the presented data are consistent with the hypothesis of a slowly developing pool of IgG4-switched memory B cells after two doses of mRNA vaccines. Furthermore, we observed significantly higher IgG4 levels after two doses of Comirnaty mRNA vaccine compared with a heterologous immunization regimen with a primary Vaxzevria vaccination followed by one dose of Comirnaty, although the total anti-spike IgG response was comparable. This argues against the hypothesis that repeated exposure to the spike protein itself triggers the unusual IgG4 response. It is currently not clear whether or to what extent the Comirnaty mRNA vaccination or the short interval of immunizations is responsible for the observed long-lasting GC reactions (12–14), but a prolonged presence of vaccine mRNA or antigen in the lymph node might be a potential explanation (12). Furthermore, a robust and persistent T follicular helper (TFH) cell response for up to 6 months after mRNA vaccination has been described in draining lymph nodes (17), which might be involved in the regulation of CSR by recurrent interactions of GC B cells with TFH cells. Of note, our study was restricted to vaccinees receiving the Comirnaty vaccine. Because the quantities and the functional profile of spike-specific antibodies induced by Comirnaty and mRNA-1273 have been reported to be slightly different (6, 34), it will be interesting to analyze whether repeated vaccination with mRNA-1273 induces a similar switch to noninflammatory IgG subclasses.Independent of the underlying mechanism, the induction of antiviral IgG4 antibodies is a phenomenon infrequently described and raises important questions about its functional consequences. Neutralizing antibodies preventing the initial binding of the viral particle to its specific cellular receptor are considered to be the most protective measure against SARS-CoV-2 infections (35). This competitive binding is mediated by the variable antigen-binding site and does not rely on the constant part of the Fc fragment. In the present study, we confirmed previous reports on improved avidity and neutralizing potential of vaccine-induced antibodies after the third vaccination (9–11). However, the large number of breakthrough infections caused by the Omicron variant indicates that current vaccination regimens do not confer sterilizing protection. Once infection is established, Fc-mediated effector functions become more relevant to clear viral infections. Systemic serology approaches have even revealed that different antibody functions can contribute to various degrees to protection dependent on the viral pathogen, as shown for influenza viruses, RSV, or SARS-CoV-2 (36–39). Passive immunization studies in animal models have further demonstrated that the degree of protection achieved by the application of mAbs depends on their IgG subclass (40–43). In this regard, IgG4 is considered an anti-inflammatory IgG with low potential to mediate Fc-dependent effector function such as ADCC or ADCP (20, 44).
High levels of antigen-specific IgG4 have been reported to correlate with successful allergen-specific immunotherapy by blocking IgE-mediated effects (45). In addition, increasing levels of bee venom–specific IgG4 have been detected in beekeepers over several beekeeping seasons and lastly even became the dominant IgG subclass for the specific antigen, i.e., phospholipase A (PLA). The IgG4 response is characterized by a very slow kinetics and takes several months to appear, whereas PLA-specific IgG1 antibodies were already measurable at earlier time points, which resembles our findings in this study (46). Furthermore, an increase in PLA-specific IgG4-switched B cells was observed in patients undergoing specific immunotherapies (SITs) (47).
So far, few studies on the role of vaccine-induced IgG4 responses against infectious diseases are available. In the field of HIV vaccine development, repeated protein immunization in the trial VAX003 (48) led to higher levels of HIV gp120-specific IgG2 and IgG4, whereas a prime-boost immunization with a canarypox vector (ALVAC-HIV) and the same protein vaccine in the RV144 trial (49) resulted in higher HIV-specific IgG3 responses correlating with partial protection against HIV (50, 51). Furthermore, the vaccine-elicited IgG3 antibodies enhanced effector functions as ADCC and ADCP, but vaccine-induced IgG4 inhibited those functions (51).With respect to the control of viral infections, little is known regarding virus-specific IgG4 antibody responses. As shown here for RSV-specific IgG responses, IgG4 is hardly induced by acute respiratory viral infections even after repeated exposure. Although measles-specific IgG4 antibodies can be induced by natural infection (52), even chronic viral infections such as human cytomegalovirus (HCMV) do not trigger significant specific IgG4 antibodies (53).
There are very few reports on the induction of IgG4 after natural infection with SARS-CoV-2. The dominant subclasses were mostly IgG1 and IgG3 (54–56).Nevertheless, a Brazilian study during the early phase of the pandemic correlated an early onset and high levels of anti-spike IgG4 antibodies with a more severe coronavirus disease 2019 (COVID-19) progression after SARS-CoV-2 infection, which might indicate a less effective antibody response (56). In addition, Della-Torre et al. (57) reported on a significant association of high IgG4/IgG1 ratios with poor disease outcome. However, in the case of a primary immune response, the causality is difficult to address because it is also possible that a more severe infection leads to an IgG4 response and not vice versa.
In our study, antibody-mediated phagocytic activity and complement deposition were reduced in sera after the third immunization, in parallel to higher proportions of anti-spike IgG4 antibodies. However, how these changes affect subsequent virus infections remains unclear. Because Fc-mediated effector function could be critical for viral clearance, an increase in IgG4 subclasses might result in longer viral persistence in case of infection. However, it is also conceivable that noninflammatory Fc-mediated effector functions reduce immunopathology, whereas virus is still being neutralized via high-avidity antibody variable regions. In a cohort of vaccinees with breakthrough infections, we did not obtain any evidence for an alteration of disease severity, which was mild in almost all of our cases. Larger cohorts with differential disease severities will be needed to address this aspect in the future. However, our results demonstrate that a subsequent infection can further boost IgG4 antibody levels, with IgG4 becoming the most dominant among all anti-spike IgG subclasses in some individuals.In summary, our study demonstrates an mRNA vaccine–induced antiviral IgG4 antibody response appearing late after secondary immunization. Further investigations are needed to clarify the precise immunological mechanisms driving this response and to evaluate whether an IgG4-driven antibody response affects subsequent viral infections and booster vaccinations. This is relevant not only for potential future vaccine campaigns against SARS-CoV-2 but also for new mRNA-based vaccine developments against other pathogens.”
Not once in your entire cut and paste does it show evidence that IgG4 Abs are known to be worse at neutralizing viral infections.
We discussed this paper when it came out. The class switch is noteworthy but I caution other readers to beware of those who throw around “highly likely” when their reference says nothing of the sort. Let’s not give into hype.
30 -
Not one antivaxxer has argued with the analysis of COVID deaths in children.
They know COVID kills kids. They just don’t care.
41 -
Harambe wrote:
Not once in your entire cut and paste does it show evidence that IgG4 Abs are known to be worse at neutralizing viral infections.
We discussed this paper when it came out. The class switch is noteworthy but I caution other readers to beware of those who throw around “highly likely” when their reference says nothing of the sort. Let’s not give into hype.
Untrue. First of all, read the entire paper. Secondly, these three paragraphs are intimating exactly that. There’s no “hype” here, just something that warrants further investigation & justifies some skepticism:
“Independent of the underlying mechanism, the induction of antiviral IgG4 antibodies is a phenomenon infrequently described and raises important questions about its functional consequences. Neutralizing antibodies preventing the initial binding of the viral particle to its specific cellular receptor are considered to be the most protective measure against SARS-CoV-2 infections (35). This competitive binding is mediated by the variable antigen-binding site and does not rely on the constant part of the Fc fragment. In the present study, we confirmed previous reports on improved avidity and neutralizing potential of vaccine-induced antibodies after the third vaccination (9–11). However, the large number of breakthrough infections caused by the Omicron variant indicates that current vaccination regimens do not confer sterilizing protection. Once infection is established, Fc-mediated effector functions become more relevant to clear viral infections. Systemic serology approaches have even revealed that different antibody functions can contribute to various degrees to protection dependent on the viral pathogen, as shown for influenza viruses, RSV, or SARS-CoV-2 (36–39). Passive immunization studies in animal models have further demonstrated that the degree of protection achieved by the application of mAbs depends on their IgG subclass (40–43). In this regard, IgG4 is considered an anti-inflammatory IgG with low potential to mediate Fc-dependent effector function such as ADCC or ADCP (20, 44).
High levels of antigen-specific IgG4 have been reported to correlate with successful allergen-specific immunotherapy by blocking IgE-mediated effects (45). In addition, increasing levels of bee venom–specific IgG4 have been detected in beekeepers over several beekeeping seasons and lastly even became the dominant IgG subclass for the specific antigen, i.e., phospholipase A (PLA). The IgG4 response is characterized by a very slow kinetics and takes several months to appear, whereas PLA-specific IgG1 antibodies were already measurable at earlier time points, which resembles our findings in this study (46). Furthermore, an increase in PLA-specific IgG4-switched B cells was observed in patients undergoing specific immunotherapies (SITs) (47).
So far, few studies on the role of vaccine-induced IgG4 responses against infectious diseases are available. In the field of HIV vaccine development, repeated protein immunization in the trial VAX003 (48) led to higher levels of HIV gp120-specific IgG2 and IgG4, whereas a prime-boost immunization with a canarypox vector (ALVAC-HIV) and the same protein vaccine in the RV144 trial (49) resulted in higher HIV-specific IgG3 responses correlating with partial protection against HIV (50, 51). Furthermore, the vaccine-elicited IgG3 antibodies enhanced effector functions as ADCC and ADCP, but vaccine-induced IgG4 inhibited those functions (51).”
03 -
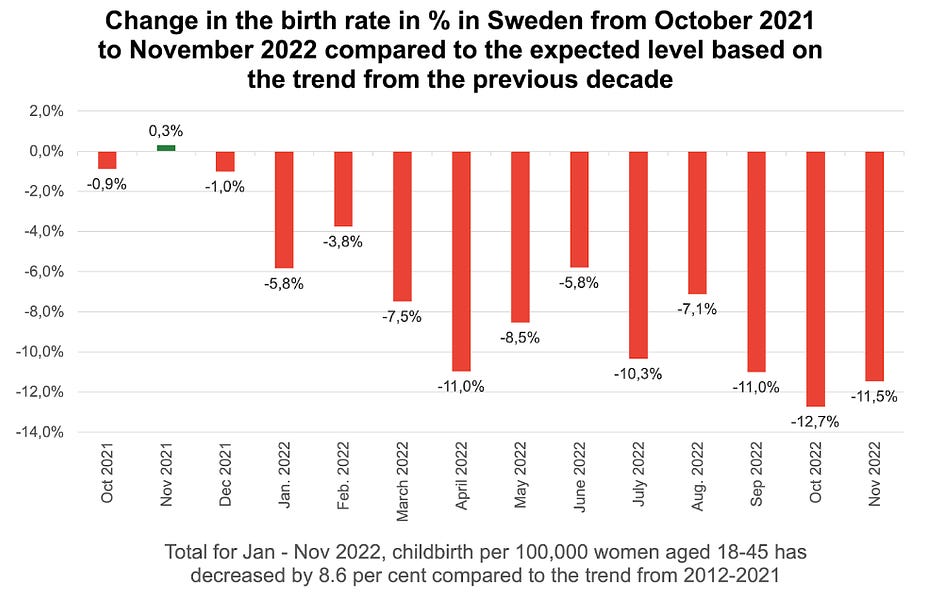
Another coincidence!
"safe & effective"
12 -
Rick Cheney wrote:
Newname wrote:
It would seem an awful lot of people have awakened and are done with these boosters.
I took two boosters and I’m probably good to go. I’ll see what emerging evidence comes out. I kind of follow Paul Offit who has been critical of boosters for young people. Please note he is very much for the vaccine. See how balanced and nuanced I am? It’s almost like I’m not an ideologue.
Yep, Offit is a pretty good one to follow. He was very skeptical of the bivalent booster and even more so when he realized our public health authorities held back data which further undermined the use of the BA4/BA5 bivalent. I’m not sure where he stands on annual boosters, but I’m guessing he’s cynical now.
Nuance is important Rick. Like some demographics absolutely needed the vaccine while others didn’t versus the risk, which is all I’ve argued from the beginning. And, of course, we had therapeutic support as well.
01