This thread was deleted by a volunteer moderator. I certainly don't want a thread this big deleted so I've restored. THat being said, this thread has served it's purpose. I've closed it to new posts.
We have a new 2024 vaccine thread here. New people don't need to try to wade through 20,000 posts to figure out what is going on.
-
42
-
Anything on BA.2.12.1 and BA.4/5 cross immunity yet?
00 -
Turtleb wrote:
At this point, especially as it seems the CDC is totally political and can't be trusted, most folks are likely to be using their own experience in deciding whether to get vaccinated.
Everyone likely personally knows dozens, if not hundreds, of individuals who've had covid and/or been vaccinated and they are going to use that data and make their decision.
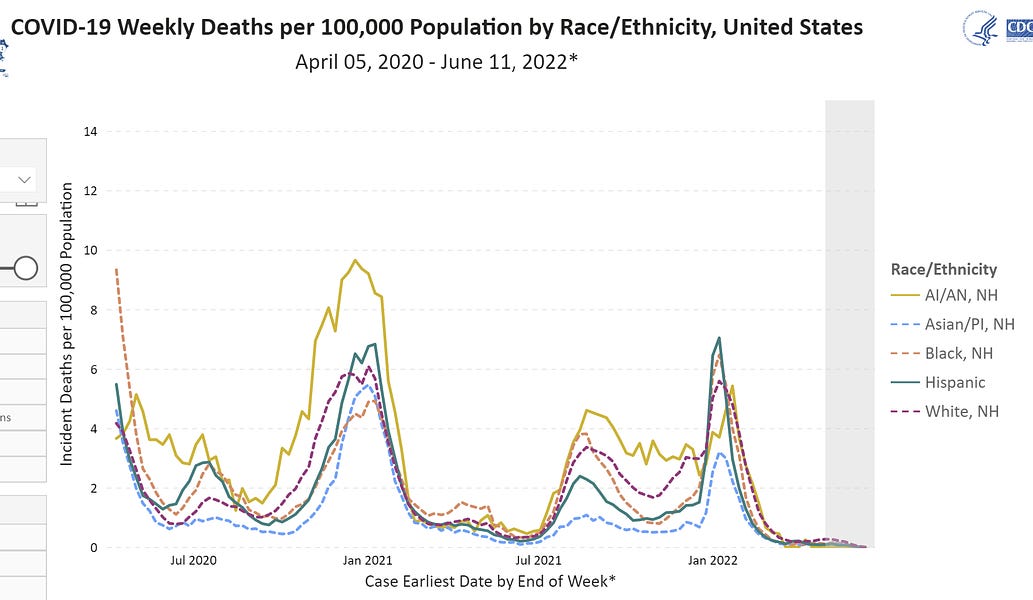
Here are the CDC death stats:
In the above plot, you tell me where vaccinations started without knowing before hand. If the vaccine actually worked as advertised, would excess deaths really not show any obvious change before and after?
Folks can see that in their everyday life and is why uptake for children and boosters is low.
“The Party told you to reject the evidence of your eyes and ears. It was their final, most essential command.”
23 -
200,000 omicron deaths?
People believe this nonsense?
22 -
44561 wrote:
As of June 2022, the Covid death rate for white Americans has recently exceeded the rates for Black, Latino and Asian Americans.
Covid has killed a smaller percentage of Black, Latino or Asian Americans over the past year than white Americans. . . .
Linked post above comes from NY Times newsletter from a couple days ago noting a higher year to date Covid death rate in white Americans vs minorities and attributes the switch to vaccination rates. Today's newsletter links a blog post from an epidemiologists that argues that the effect might better be explained by group age disparities. That is a Simpson's paradox issue as has been discussed ad nauseum in this thread. In any case the relative rates between the groups does seem to have shifted.
00 -
Monkeys Skyping wrote:
44561 wrote:
As of June 2022, the Covid death rate for white Americans has recently exceeded the rates for Black, Latino and Asian Americans.
Covid has killed a smaller percentage of Black, Latino or Asian Americans over the past year than white Americans. . . .
Linked post above comes from NY Times newsletter from a couple days ago noting a higher year to date Covid death rate in white Americans vs minorities and attributes the switch to vaccination rates. Today's newsletter links a blog post from an epidemiologists that argues that the effect might better be explained by group age disparities. That is a Simpson's paradox issue as has been discussed ad nauseum in this thread. In any case the relative rates between the groups does seem to have shifted.
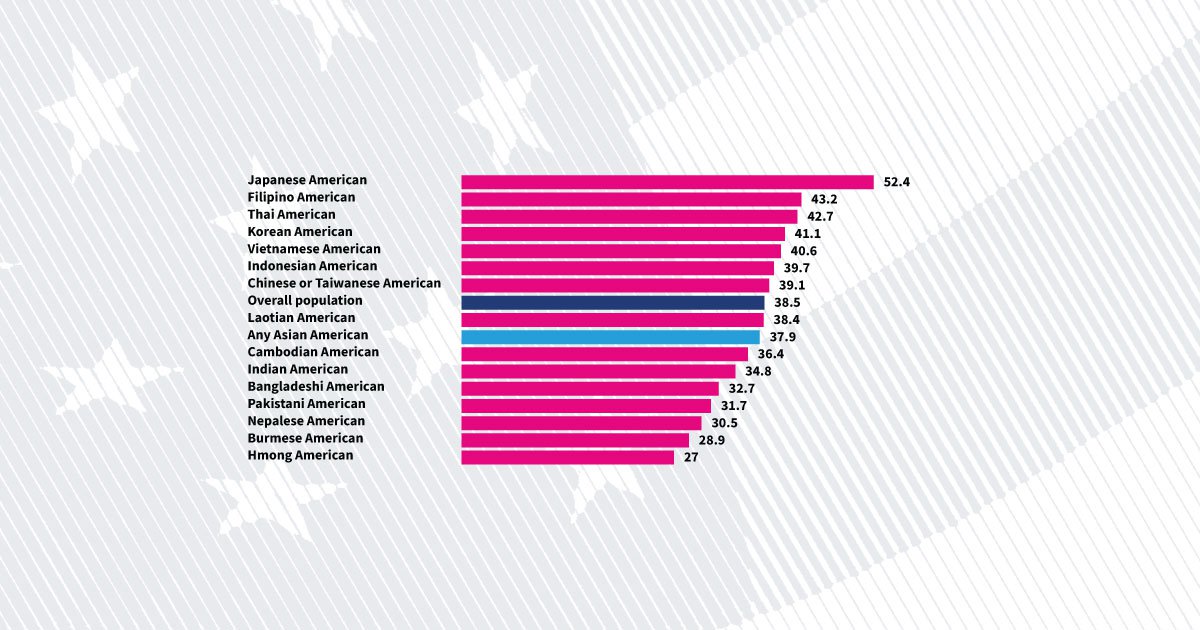
Fact remains that the most highly vaxxed ethnic group in America has a higher Covid death rate than any other ethnic group.
Can't we reasonably conclude from that fact that the vaxxes are not preventing deaths very effectively?
By the way, are White Americans as a group older on average than Asian Americans?
61 -
So the vitamin C works against sepsis theory is wrong.
Who cares? Well this is a good example of
1) smaller, poorer quality RCTs not being useful for much beyond justifying a larger study. Just like with IVM, small, early, and less rigorous studies showed a possible effect. The obvious thing was to wait until we had big RCT data to form an opinion. Nobody here is going to rabidly defend vitamin C for sepsis now that we have conclusive data. Or maybe they will?
2) “It can’t hurt” is often tragically wrong. There was a statistically significant INCREASE in death or organ dysfunction in the vitamin C arm of the trial. Even something as commonplace as vitamin C can be harmful with the right dose and the wrong health background.
06 -
Harambe blows dudes confirmed.
41 -
Harambe wrote:
So the vitamin C works against sepsis theory is wrong.Who cares? Well this is a good example of
1) smaller, poorer quality RCTs not being useful for much beyond justifying a larger study. Just like with IVM, small, early, and less rigorous studies showed a possible effect. The obvious thing was to wait until we had big RCT data to form an opinion. Nobody here is going to rabidly defend vitamin C for sepsis now that we have conclusive data. Or maybe they will?
2) “It can’t hurt” is often tragically wrong. There was a statistically significant INCREASE in death or organ dysfunction in the vitamin C arm of the trial. Even something as commonplace as vitamin C can be harmful with the right dose and the wrong health background.
+1 good points
06 -
Beau Biden is dead ha ha wrote:
Harambe blows dudes confirmed.
Repressed right winger confirmed
15 -
antivaxxers killing democracy - - - - - wrote:
Beau Biden is dead ha ha wrote:
Harambe blows dudes confirmed.
Repressed right winger confirmed
Proud fudgepacker confirmed.
Also, how are you doing? Hope things are going well in your life.
21 -
It's funny this thread has died because the all of anti-vaxxers conspiracy theories have flatten completely flat. The past few months were supposed to be "the proof," but the vaccines continue to be exceptionally effective at stopping people from dying.
16 -
2600 bro wrote:
It's funny this thread has died because the all of anti-vaxxers conspiracy theories have flatten completely flat. The past few months were supposed to be "the proof," but the vaccines continue to be exceptionally effective at stopping people from dying.
What is funny is that you "and" Harambe "both" stopped posting for 5 days, and now you are "both" back posting within minutes of each other.
Really funny...
81 -
Tthh wrote:
2600 bro wrote:
It's funny this thread has died because the all of anti-vaxxers conspiracy theories have flatten completely flat. The past few months were supposed to be "the proof," but the vaccines continue to be exceptionally effective at stopping people from dying.
What is funny is that you "and" Harambe "both" stopped posting for 5 days, and now you are "both" back posting within minutes of each other.
Really funny...
Could it be, I am just overjoyed when Harambe choke-slams anti-vaxxers and, thus, cannot resist poasting when this thread returns to the front page.
BTW... your post proves my point. TY :)
17 -
2600 bro wrote:
Tthh wrote:
What is funny is that you "and" Harambe "both" stopped posting for 5 days, and now you are "both" back posting within minutes of each other.
Really funny...
Could it be, I am just overjoyed when Harambe choke-slams anti-vaxxers and, thus, cannot resist poasting when this thread returns to the front page.
BTW... your post proves my point. TY :)
It doesn't prove your point because I am not antivaxx.
Your move, moron :)
60 -
Latest installment of data from one of the largest hospital systems in MI:
Hospitalized- 62 Unvax, 84 Vax (45 Boosted!)
In ICU- 3 Unvax, 9 Vax (6 Boosted!)
On ventilator- 2 Unvax, 5 Vax (3 Boosted!)
Do the boosters GIVE you Covid?! LOL
30 -
Harambe wrote:
So the vitamin C works against sepsis theory is wrong.Who cares? Well this is a good example of
1) smaller, poorer quality RCTs not being useful for much beyond justifying a larger study. Just like with IVM, small, early, and less rigorous studies showed a possible effect. The obvious thing was to wait until we had big RCT data to form an opinion. Nobody here is going to rabidly defend vitamin C for sepsis now that we have conclusive data. Or maybe they will?
2) “It can’t hurt” is often tragically wrong. There was a statistically significant INCREASE in death or organ dysfunction in the vitamin C arm of the trial. Even something as commonplace as vitamin C can be harmful with the right dose and the wrong health background.
Thanks for posting this, but my takeaway from the study is a bit different.
Let me give an analogy. If you drive a car that's low in oil for tens of thousands of miles, a lot of bad things can happen. If you wait until one of those bad thing happens (worn rings, for example), you can't bring the oil level up to normal and expect it to cure that bad thing.
These patients were VERY sick... and age 65±14. They were already in ICU before IVM was started. 40% died regardless of treatment. By six months, 46% and 43% of the vitC and control group had died. We don't know what the quality of life was during those last months of life.
Thus, this was a pretty narrow study. I agree that it proves that IV vitamin C in 1) the dosage used 2) after sepsis progressed to ICU admission 3) in an old patient with chronically low vit C levels isn't beneficial and might be worse than no action.
I'm not a strong proponent of IVM, but I am extremely disappointed with the hatchet job that IVM has been given by the media and medical researchers.
Here is my beef with IVM research.
In spite of the massive interest that IVM has generated, I have yet to see an IVM study that follows FLCCC protocol. Specifically, 1)Start IVM within 5 days of first symptom. 2) Continue for a minimum of 5 days or until symptoms are gone 3) given at the recommended doses and 4) Insure zinc levels are adequate or supplement as needed. This is where the observational studies have succeeded with IVM.
In every IVM study I've read, IVM is started too late, not continued for 5 days, not given in the dose recommended, and zinc levels have not been supplemented.
I'm a layman with no research background, yet I can find this protocol with a simple search.
Why isn't the recommended protocol being tested? I can't find a single IVM study that follows the protocol that front line doctors have used successfully.
Let me end with another analogy. In 1940, Howard Florey did his first human test of penicillin on Albert Alexander, who had sepsis. The patient recovered, but after five days, penicillin treatment stopped because Florey ran out of penicillin. The patient relapsed and died. Florey accurately deduced that given sooner or given longer, penicillin would have been successful. I'm not suggesting that vit C would have cured these patients. I'm pointing out that researchers setting up IVM studies, for some unknown reason, lack the ability to learn from medical history. Florey "observed" what worked... and millions of lives were saved.
IVM *might* be a decent therapy. It might not. Doctors should be allowed to prescribe it until we find out. We can just agree to disagree on that point.
10 -
The vaccine has turned me trans and george bush did 9/11.
10 -
seems they're finding all kinds of strange formations in the deceased, weird looking blood clot things
10 -
Heartlesss wrote:
Latest installment of data from one of the largest hospital systems in MI:
Hospitalized- 62 Unvax, 84 Vax (45 Boosted!)
In ICU- 3 Unvax, 9 Vax (6 Boosted!)
On ventilator- 2 Unvax, 5 Vax (3 Boosted!)
--------------------------------------------------------------------------------
This would be more interesting if we could know what percentage of the relevant age group(s) in that area had been vaccinated/boosted. Random-number example: If 90% have been vaccinated and boosted, but the unvaccinated 10% constitute a quarter or more of those hospitalized/intubated, we could--if the population is large enough--reasonably conclude that the vaccines were helpful.
I don't know the numbers of vaccinated/boosted in MI, but I know that in NYC only 2% of residents over age 18 are completely unvaccinated. So if the unvaccinated in a given age group constitute something larger than 2%, especially something significantly larger, it's reasonable to conclude that vaccination may confer a major benefit.
Fortunately, we have good data for recent trends in NYC. As of 5/21 (data are incomplete for more recent weeks), the weekly age-adjusted death rate per 100,000 for those who are vaccinated and boosted was .25; for those who were vaccinated but not boosted, .41; and for those not vaccinated, 12.24--nearly 49 times the rate for those who were vaccinated and boosted.
NOTE that we should not necessarily give the vaccines and boosters *all* the credit, as those who have not been vaccinated are more likely--on average--to have other behaviors/conditions that would predispose toward bad outcomes.
01