This thread was deleted by a volunteer moderator. I certainly don't want a thread this big deleted so I've restored. THat being said, this thread has served it's purpose. I've closed it to new posts.
We have a new 2024 vaccine thread here. New people don't need to try to wade through 20,000 posts to figure out what is going on.
Pfizer stood by the 95% RRR stat in their clinical trial... because it was true. Paxton being a moron and trying to claim everything should be stated as ARR is like preschool level statistics.
Nice try. You clearly didnt read/comprehend.
The document linked below on the FDA site, “Communicating Risks and Benefits,” suggests to “Provide absolute risks, not just relative risks.” It’s relatively easy to clearly provide both with equal prominence. It’s easy to provide examples where just providing one or the other would be deceptive.
It makes researchers appear as pharma shills when they just provide relative risk and that inevitably gets picked up in a press release. Better to increase trust by providing both, in my opinion.
Relative risks matter A LOT. Protecting against rare, but severe outcomes is something most people want!
The original publication reports all the data you want - I have linked it many many times. Just because you refuse to read it, and demand things be simplified and re-processed to fit your priors doesn't mean much.
The document linked below on the FDA site, “Communicating Risks and Benefits,” suggests to “Provide absolute risks, not just relative risks.” It’s relatively easy to clearly provide both with equal prominence. It’s easy to provide examples where just providing one or the other would be deceptive.
It makes researchers appear as pharma shills when they just provide relative risk and that inevitably gets picked up in a press release. Better to increase trust by providing both, in my opinion.
Relative risks matter A LOT. Protecting against rare, but severe outcomes is something most people want!
The original publication reports all the data you want - I have linked it many many times. Just because you refuse to read it, and demand things be simplified and re-processed to fit your priors doesn't mean much.
Lots of name-calling. I guess you didn’t read what I wrote. I didn’t say relative risk doesn’t matter. Even though the document at the FDA suggests to use absolute risk, I suggest to use *both* with *equal prominence.*
Relative risks matter A LOT. Protecting against rare, but severe outcomes is something most people want!
The original publication reports all the data you want - I have linked it many many times. Just because you refuse to read it, and demand things be simplified and re-processed to fit your priors doesn't mean much.
Lots of name-calling. I guess you didn’t read what I wrote. I didn’t say relative risk doesn’t matter. Even though the document at the FDA suggests to use absolute risk, I suggest to use *both* with *equal prominence.*
The document isn't even FDA guidelines, it's just an FDA sponsored compendium of essays trying to educate physicians and scientists on communication.
But try this:
Think about it in the context of a vaccine for a disease with poor epidemiology data; you don't really know the short, medium, or long term chance of infection, risk of severe disease/death, etc.
Secondly, even without precise data, people already have a pretty firm estimate of what the chance of COVID infection is, everyone was getting it left and right, it wasn't some rare event.
Relative risk communicates a lot more here, and is very helpful for people understand.
If it's something like a study reporting on the effect of 100mpw training on preventing chordoma on your offspring, it makes a lot more sense to report absolute risk because the lay-person probably doesnt know that chordoma has a ~1 in 1,000,000 incidence rate.
Pfizer stood by the 95% RRR stat in their clinical trial... because it was true. Paxton being a moron and trying to claim everything should be stated as ARR is like preschool level statistics.
Nice try. You clearly didnt read/comprehend.
The document linked below on the FDA site, “Communicating Risks and Benefits,” suggests to “Provide absolute risks, not just relative risks.” It’s relatively easy to clearly provide both with equal prominence. It’s easy to provide examples where just providing one or the other would be deceptive.
It makes researchers appear as pharma shills when they just provide relative risk and that inevitably gets picked up in a press release. Better to increase trust by providing both, in my opinion.
Communicating the more useful measure of risk doesn't make anyone a shill.
It's much easier for people to understand "95+% less likely to die of COVID" than showing them two smaller numbers.
Besides, the CDC regularly published mortality stats. Many states had public dashboards showing COVID risks by age/sex/etc. Relative risks were well communicated!
The data were all out there. Relative risk is what people are used to and skilled at interpreting: Drug A reduced the risk of stroke by 75%, etc.
Lots of name-calling. I guess you didn’t read what I wrote. I didn’t say relative risk doesn’t matter. Even though the document at the FDA suggests to use absolute risk, I suggest to use *both* with *equal prominence.*
The document isn't even FDA guidelines, it's just an FDA sponsored compendium of essays trying to educate physicians and scientists on communication.
But try this:
Think about it in the context of a vaccine for a disease with poor epidemiology data; you don't really know the short, medium, or long term chance of infection, risk of severe disease/death, etc.
Secondly, even without precise data, people already have a pretty firm estimate of what the chance of COVID infection is, everyone was getting it left and right, it wasn't some rare event.
Relative risk communicates a lot more here, and is very helpful for people understand.
If it's something like a study reporting on the effect of 100mpw training on preventing chordoma on your offspring, it makes a lot more sense to report absolute risk because the lay-person probably doesnt know that chordoma has a ~1 in 1,000,000 incidence rate.
I didn't say it was official FDA guidance. Both Absolute Risk and Relative Risk provide useful information. Relative Risk communicates useful information if the symptom is very common, but if it's relatively rare (even much more common than your 1 in 1,000,000 incident rate example), then absolute risk is very important. That is why I suggest both. It avoids the appearance of bias. The new CDC Director wants to rebuild trust. If she's really serious about that, she would get rid of personnel who fabricated numbers for the NEJM, stop arguing in court to hide their anonymized database information for 50+ years and also commit to show both relative risk and absolute risk with equal prominence. If she doesn't, don't be shocked if there is continued increase in distrust in medical science.
This post was edited 4 minutes after it was posted.
The document isn't even FDA guidelines, it's just an FDA sponsored compendium of essays trying to educate physicians and scientists on communication.
But try this:
Think about it in the context of a vaccine for a disease with poor epidemiology data; you don't really know the short, medium, or long term chance of infection, risk of severe disease/death, etc.
Secondly, even without precise data, people already have a pretty firm estimate of what the chance of COVID infection is, everyone was getting it left and right, it wasn't some rare event.
Relative risk communicates a lot more here, and is very helpful for people understand.
If it's something like a study reporting on the effect of 100mpw training on preventing chordoma on your offspring, it makes a lot more sense to report absolute risk because the lay-person probably doesnt know that chordoma has a ~1 in 1,000,000 incidence rate.
I didn't say it was official FDA guidance. Both Absolute Risk and Relative Risk provide useful information. Relative Risk communicates useful information if the symptom is very common, but if it's relatively rare (even much more common than your 1 in 1,000,000 incident rate example), then absolute risk is very important. That is why I suggest both. It avoids the appearance of bias. The new CDC Director wants to rebuild trust. If she's really serious about that, she would get rid of personnel who fabricated numbers for the NEJM, stop arguing in court to hide their anonymized database information for 50+ years and also commit to show both relative risk and absolute risk with equal prominence. If she doesn't, don't be shocked if even there is continued increase in distrust in medical science.
I am sorry do you really there is a case for forgoing COVID vaccines because of absolute risk reduction, given the near zero cost (time, adverse events, monetary cost) of the vaccine?
The CDC director has nothing to do with clinical trials overseen by the FDA, nor manuscripts published in NJEM...
I didn't say it was official FDA guidance. Both Absolute Risk and Relative Risk provide useful information. Relative Risk communicates useful information if the symptom is very common, but if it's relatively rare (even much more common than your 1 in 1,000,000 incident rate example), then absolute risk is very important. That is why I suggest both. It avoids the appearance of bias. The new CDC Director wants to rebuild trust. If she's really serious about that, she would get rid of personnel who fabricated numbers for the NEJM, stop arguing in court to hide their anonymized database information for 50+ years and also commit to show both relative risk and absolute risk with equal prominence. If she doesn't, don't be shocked if even there is continued increase in distrust in medical science.
I am sorry do you really there is a case for forgoing COVID vaccines because of absolute risk reduction, given the near zero cost (time, adverse events, monetary cost) of the vaccine?
The CDC director has nothing to do with clinical trials overseen by the FDA, nor manuscripts published in NJEM...
The CDC Director has the ability to eliminate their own personnel who fabricated numbers in a study they published in the New England Journal of Medicine, especially if one of those persons leads their COVID team. That would be a start for rebuilding trust along with the other things I mentioned. There are countless people hearing about things such as what I mentioned and that is what I suggest as a *start* to rebuild trust. If she just wants to go around and appear on news shows promoting drugs suggested by the CDC, that's okay too as I'll keep sharing information that I think is helpful. (And I know people who disagree with me will share information as well to try and be helpful in their own way. I can understand that.)
This post was edited 7 minutes after it was posted.
I am sorry do you really there is a case for forgoing COVID vaccines because of absolute risk reduction, given the near zero cost (time, adverse events, monetary cost) of the vaccine?
The CDC director has nothing to do with clinical trials overseen by the FDA, nor manuscripts published in NJEM...
The CDC Director has the ability to eliminate their own personnel who fabricated numbers in a study they published in the New England Journal of Medicine, especially if one of those persons leads their COVID team. That would be a start for rebuilding trust along with the other things I mentioned. There are countless people hearing about things such as what I mentioned and that is what I suggest as a *start* to rebuild trust. If she just wants to go around and appear on news shows promoting drugs suggested by the CDC, that's okay too as I'll keep sharing information that I think is helpful. (And I know people who disagree with me will share information as well to try and be helpful in their own way. I can understand that.)
What fraudulent study did the CDC publish in NJEM? News to me.
Pfizer stood by the 95% RRR stat in their clinical trial... because it was true. Paxton being a moron and trying to claim everything should be stated as ARR is like preschool level statistics.
Nice try. You clearly didnt read/comprehend.
The document linked below on the FDA site, “Communicating Risks and Benefits,” suggests to “Provide absolute risks, not just relative risks.” It’s relatively easy to clearly provide both with equal prominence. It’s easy to provide examples where just providing one or the other would be deceptive.
It makes researchers appear as pharma shills when they just provide relative risk and that inevitably gets picked up in a press release. Better to increase trust by providing both, in my opinion.
Absolute risk isn't time stationary because infection rates are not time stationary, so it's silly to point to that as an important metric from the vaccine trials.
As a policy metric it can be useful in guiding the recommendations for when and who ought to be getting vaccinated and/or boosted, which is what is being done.
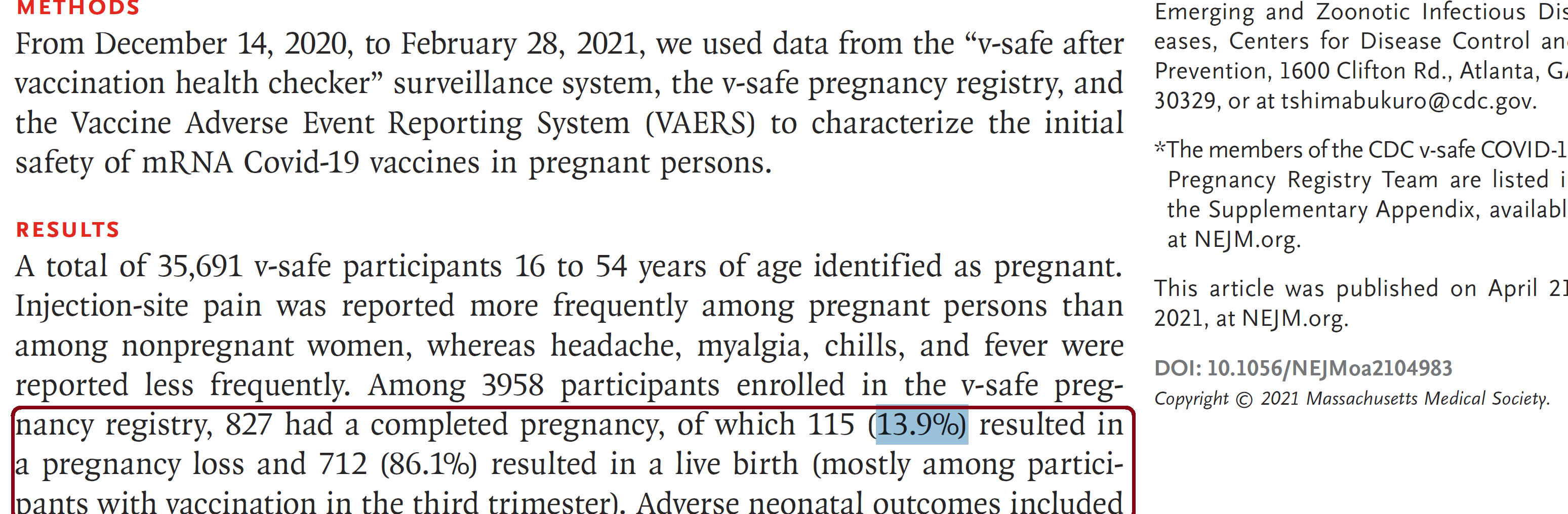
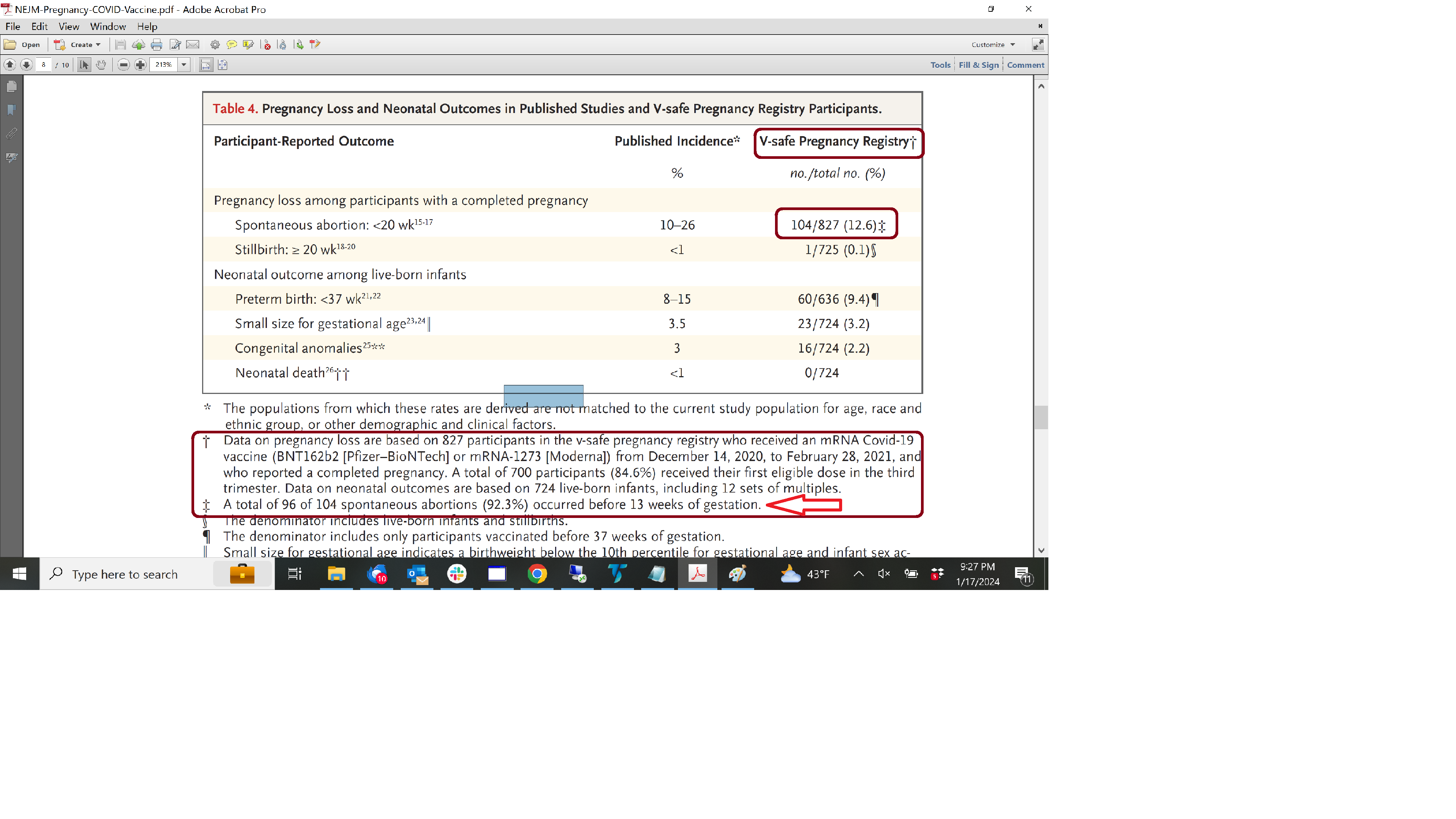
They said that only 13.9% of the subjects experienced a pregnancy loss. That was a made up number and obvious to anyone who read the paper. Almost every subject was enrolled in the study after the study’s cutoff for pregnancy loss. Other numbers in that table (Table 4) were also deceptive at best. It was amazing that so many CDC & FDA scientists would publish such nonsense and the NEJM didn’t catch it.
The majority of the paper was about pregnancy loss and covid drugs (since that was the biggest issue regarding pregnancy in VAERS). After being brow-beaten on the Internet and someone writing NEJM, they changed the paper months later to be only about 3rd trimester pregnancy and covid drugs. That’s what is on NEJM now.
There are other serious issues in this study such as a glaringly obvious safety signal for birth defects based on data from this study and from other CDC’s research as well as the use of a database that is hidden from the public and corrupted with bias by letting the subjects know during the testing phase that the test drug is “safe & effective.” The CDC published a followup study that changed the definitions of trimesters(!) making numerical comparisons between this study and the followup study nearly impossible.
The only reason we know about the bogus numbers in Table 4 is because it was a pregnancy study. Had they put bogus numbers in some of their other studies, it would likely be undetectable. This is why getting rid of these people (or keeping them from CDC research and decision-making) is important for the public trust. I want people to have faith in CDC scientists, but only if they’re ethical and competent.
Happy to go into more detail about this study and can probably locate an image of the original Table 4.
They said that only 13.9% of the subjects experienced a pregnancy loss. That was a made up number and obvious to anyone who read the paper. Almost every subject was enrolled in the study after the study’s cutoff for pregnancy loss. Other numbers in that table (Table 4) were also deceptive at best. It was amazing that so many CDC & FDA scientists would publish such nonsense and the NEJM didn’t catch it.
The majority of the paper was about pregnancy loss and covid drugs (since that was the biggest issue regarding pregnancy in VAERS). After being brow-beaten on the Internet and someone writing NEJM, they changed the paper months later to be only about 3rd trimester pregnancy and covid drugs. That’s what is on NEJM now.
There are other serious issues in this study such as a glaringly obvious safety signal for birth defects based on data from this study and from other CDC’s research as well as the use of a database that is hidden from the public and corrupted with bias by letting the subjects know during the testing phase that the test drug is “safe & effective.” The CDC published a followup study that changed the definitions of trimesters(!) making numerical comparisons between this study and the followup study nearly impossible.
The only reason we know about the bogus numbers in Table 4 is because it was a pregnancy study. Had they put bogus numbers in some of their other studies, it would likely be undetectable. This is why getting rid of these people (or keeping them from CDC research and decision-making) is important for the public trust. I want people to have faith in CDC scientists, but only if they’re ethical and competent.
Happy to go into more detail about this study and can probably locate an image of the original Table 4.
Calling this fraud is a huge stretch. Seems like sloppy statistics at worst. But it's easy to assume malicious intent when someone holds an opposing point of view....
There have been many studies on vaccine safety during pregnancy. Here's a meta-analysis:
Assessment of COVID-19 vaccines safety during pregnancy is urgently needed.We conducted a systematic review and meta-analysis to evaluate the safety of COVID-19 vaccines, including their components and technological platforms...
They said that only 13.9% of the subjects experienced a pregnancy loss. That was a made up number and obvious to anyone who read the paper. Almost every subject was enrolled in the study after the study’s cutoff for pregnancy loss. Other numbers in that table (Table 4) were also deceptive at best. It was amazing that so many CDC & FDA scientists would publish such nonsense and the NEJM didn’t catch it.
The majority of the paper was about pregnancy loss and covid drugs (since that was the biggest issue regarding pregnancy in VAERS). After being brow-beaten on the Internet and someone writing NEJM, they changed the paper months later to be only about 3rd trimester pregnancy and covid drugs. That’s what is on NEJM now.
There are other serious issues in this study such as a glaringly obvious safety signal for birth defects based on data from this study and from other CDC’s research as well as the use of a database that is hidden from the public and corrupted with bias by letting the subjects know during the testing phase that the test drug is “safe & effective.” The CDC published a followup study that changed the definitions of trimesters(!) making numerical comparisons between this study and the followup study nearly impossible.
The only reason we know about the bogus numbers in Table 4 is because it was a pregnancy study. Had they put bogus numbers in some of their other studies, it would likely be undetectable. This is why getting rid of these people (or keeping them from CDC research and decision-making) is important for the public trust. I want people to have faith in CDC scientists, but only if they’re ethical and competent.
Happy to go into more detail about this study and can probably locate an image of the original Table 4.
Nothing is scrubbed or hidden. The correction is right here:
Calling this fraud is a huge stretch. Seems like sloppy statistics at worst. But it's easy to assume malicious intent when someone holds an opposing point of view....
There have been many studies on vaccine safety during pregnancy. Here's a meta-analysis:
The fact that you say there is a 'glaringly obvious' signal for birth defects suggests there's some motivated reasoning here.
The data was fabricated on the number related to pregnancy loss. It wasn't statistical errors, but a number that was just made up for data that didn't exist and couldn't possibly exist. I think it was deliberate fabrication as I don't see how so many CDC and FDA authors would accidently make up a number for pregnancy loss. But whether it is deliberate or incompetence, it is clear that these authors need to be removed from the CDC and FDA (or at least reassigned) in order to regain any trust. It was a really bad look for the lead author to keep the position of running the CDC's response to COVID. Obviously, all of the sources of data used by the CDC need to be made public in an anonymized fashion to regain trust rather than people forcing them to do so in court.
As far as the "glaringly obvious" signal for birth defects, it is very simple. One of the common symptoms listed in this study was shown by another CDC researcher in a 2017 paper to increase the risk factor of a certain type of birth defect. The CDC refused to even send out an alert for pregnant women.
The meta analysis includes databases that are hidden from the public and other scientists. The larger one by Kharbanda includes data from the Vaccine Safety Datalink (VSD) database -- which is one that has yet to be released. "V-Safe" database data (for example) has to be released starting 2/15/2024 by a recent court order. As far as I know, VSD data is still hidden. The VSD data was used by the CDC to underestimate anaphylactic reactions by 50-100 times. We only got a more accurate estimate of these types of reactions to certain COVID vaccine drugs when independent research was conducted. So, anything that comes from hidden VSD data is not going to be trusted by many people until the actual data is released.
It all comes down to trust issues with the CDC and there are so many things with fabricating data, avoiding to provide alerts to people when the data and potential danger is known (and not just for birth defects), hiding anonymized data from scientists and the public, etc.
Help us build the best running shoe review site for a chance to win a LetsRun t-shirt.Help us build the best running shoe review site for a chance to win one of 10 LetsRun t-shirts.