This thread was deleted by a volunteer moderator. I certainly don't want a thread this big deleted so I've restored. THat being said, this thread has served it's purpose. I've closed it to new posts.
We have a new 2024 vaccine thread here. New people don't need to try to wade through 20,000 posts to figure out what is going on.
-
05
-
2600 bro wrote:
DanM wrote:
Crazy people like Charlie Munger wanted to force it on us.
“If I were running the world, of course it would be mandatory,” Munger said. “When I was in World War Two’s army, they didn’t ask me if I wanted a vaccination. They just vaccinated me. It didn’t hurt me or anybody else in that world. We all just submitted to whatever the government told us to submit to.
Completely random response too.
DanM is going downhill - sad to see.
YOU and YOUR GANG are the ones going downhill.
News of another victory:
63 -
Devil horns on Fauci on Time Magazine cover in 2020!
43 -
A U.S. Navy Medical Officer exposes a startling increase in heart-related problems among military pilots following COVID-19 vaccination, according to Defense Department data.
Recent developments have brought to light concerning statistics regarding the health of military pilots post-COVID-19 vaccination. Lieutenant Ted Macie, an active-duty officer in the Navy Medical Service Corps and a whistleblower, has revealed Department of Defense data showing a significant rise in heart-related issues among pilots following their COVID-19 vaccination.Lt. Macie, also serving as a Navy Health Administrator and Medical Recruiter, disclosed these findings in a video, building upon concerns initially raised by his wife, Mara Macie, a candidate for Florida’s 5th Congressional District. Mara Macie’s social media post had previously criticized the handling of service members during the vaccine rollout, underscoring a deep-seated mistrust in military leadership and calling for accountability.
The data presented by Lt. Macie indicates alarming increases in various heart-related ailments among both fixed-wing and helicopter pilots. The statistics show surges in conditions like hypertensive disease (up by 36%), ischemic heart disease (up by 69%), pulmonary heart disease (up by 62%), heart failure (up by 973%), other forms of heart disease (up by 63%), and cardiomyopathy (up by 152%) compared to the five-year average prior to 2022.
This revelation follows a report by The Gateway Pundit in July, citing a military study that acknowledged a spike in myocarditis cases by at least 151% post-vaccination in the US Military. Gilbert Cisneros Jr., the Undersecretary of Defense for Personnel and Readiness, confirmed an increase in myocarditis cases, with 275 reported in 2021, significantly higher than the annual average from 2016 to 2020.
63 -
Newname wrote:
Devil horns on Fauci on Time Magazine cover in 2020!
Youve convinced me
33 -
Newname wrote:
A U.S. Navy Medical Officer exposes a startling increase in heart-related problems among military pilots following COVID-19 vaccination, according to Defense Department data.
Recent developments have brought to light concerning statistics regarding the health of military pilots post-COVID-19 vaccination. Lieutenant Ted Macie, an active-duty officer in the Navy Medical Service Corps and a whistleblower, has revealed Department of Defense data showing a significant rise in heart-related issues among pilots following their COVID-19 vaccination.
Lt. Macie, also serving as a Navy Health Administrator and Medical Recruiter, disclosed these findings in a video, building upon concerns initially raised by his wife, Mara Macie, a candidate for Florida’s 5th Congressional District. Mara Macie’s social media post had previously criticized the handling of service members during the vaccine rollout, underscoring a deep-seated mistrust in military leadership and calling for accountability.
The data presented by Lt. Macie indicates alarming increases in various heart-related ailments among both fixed-wing and helicopter pilots. The statistics show surges in conditions like hypertensive disease (up by 36%), ischemic heart disease (up by 69%), pulmonary heart disease (up by 62%), heart failure (up by 973%), other forms of heart disease (up by 63%), and cardiomyopathy (up by 152%) compared to the five-year average prior to 2022.
This revelation follows a report by The Gateway Pundit in July, citing a military study that acknowledged a spike in myocarditis cases by at least 151% post-vaccination in the US Military. Gilbert Cisneros Jr., the Undersecretary of Defense for Personnel and Readiness, confirmed an increase in myocarditis cases, with 275 reported in 2021, significantly higher than the annual average from 2016 to 2020.
This meshes perfectly well with the data showing decreasing service member out of combat deaths in 2021 and 2022 and 2023.
62 -
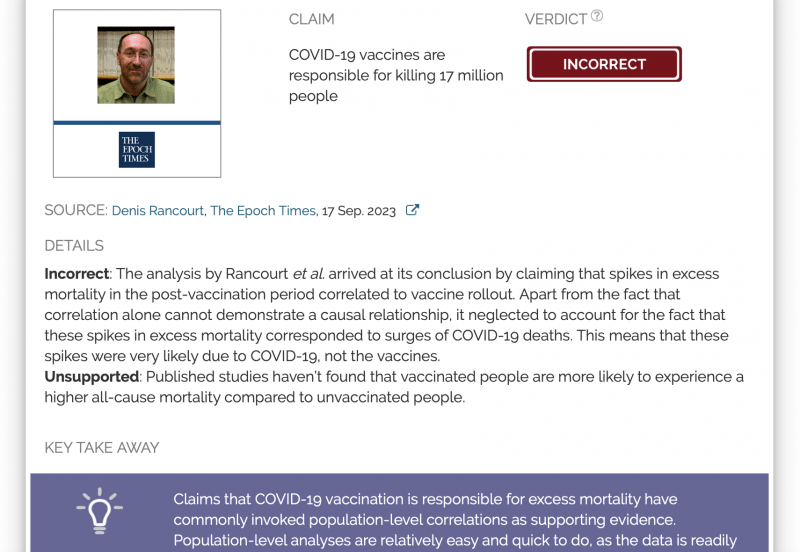
Seventeen equatorial and Southern-Hemisphere countries were studied (Argentina, Australia, Bolivia, Brazil, Chile, Colombia, Ecuador, Malaysia, New Zealand, Paraguay, Peru, Philippines, Singapore, South Africa, Suriname, Thailand, Uruguay), which comprise 9.10 % of worldwide population, 10.3 % of worldwide COVID-19 injections (vaccination rate of 1.91 injections per person, all ages), virtually every COVID-19 vaccine type and manufacturer, and span 4 continents.
In the 17 countries, there is no evidence in all-cause mortality (ACM) by time data of any beneficial effect of COVID-19 vaccines. There is no association in time between COVID-19 vaccination and any proportionate reduction in ACM. The opposite occurs.
All 17 countries have transitions to regimes of high ACM, which occur when the COVID-19 vaccines are deployed and administered. Nine of the 17 countries have no detectable excess ACM in the period of approximately one year after a pandemic was declared on 11 March 2020 by the World Health Organization (WHO), until the vaccines are rolled out (Australia, Malaysia, New Zealand, Paraguay, Philippines, Singapore, Suriname, Thailand, Uruguay). Unprecedented peaks in ACM occur in the summer (January-February) of 2022 in the Southern Hemisphere, and in equatorial-latitude countries, which are synchronous with or immediately preceded by rapid COVID-19-vaccine-booster-dose rollouts (3rd or 4th doses). This phenomenon is present in every case with sufficient mortality data (15 countries).
Two of the countries studied have insufficient mortality data in January- February 2022 (Argentina and Suriname). Detailed mortality and vaccination data for Chile and Peru allow resolution by age and by dose number. It is unlikely that the observed peaks in all-cause mortality in January- February 2022 (and additionally in: July-August 2021, Chile; July-August 2022, Peru), in each of both countries and in each elderly age group, could be due to any cause other than the temporally associated rapid COVID-19-vaccine-booster-dose rollouts.
Likewise, it is unlikely that the transitions to regimes of high ACM, coincident with the rollout and sustained administration of COVID-19 vaccines, in all 17 Southern- Hemisphere and equatorial-latitude countries, could be due to any cause other than the vaccines. Synchronicity between the many peaks in ACM (in 17 countries, on 4 continents, in all elderly age groups, at different times) and associated rapid booster rollouts allows this firm conclusion regarding causality, and accurate quantification of COVID-19-vaccine toxicity. The all-ages vaccine-dose fatality rate (vDFR), which is the ratio of inferred vaccine- induced deaths to vaccine doses delivered in a population, is quantified for the January- February 2022 ACM peak to fall in the range 0.02 % (New Zealand) to 0.20 % (Uruguay). In Chile and Peru, the vDFR increases exponentially with age (doubling approximately every 4 years of age), and is largest for the latest booster doses, reaching approximately 5 % in the 90+ years age groups (1 death per 20 injections of dose 4). Comparable results occur for the Northern Hemisphere, as found in previous articles (India, Israel, USA). We quantify the overall all-ages vDFR for the 17 countries to be (0.126 ± 0.004) %, which would imply 17.0 ± 0.5 million COVID-19 vaccine deaths worldwide, from 13.50 billion injections up to 2 September 2023. This would correspond to a mass iatrogenic event that killed (0.213 ± 0.006) % of the world population (1 death per 470 living persons, in less than 3 years), and did not measurably prevent any deaths. The overall risk of death induced by injection with the COVID-19 vaccines in actual populations, inferred from excess all-cause mortality and its synchronicity with rollouts, is globally pervasive and much larger than reported in clinical trials, adverse effect monitoring, and cause-of-death statistics from death certificates, by 3 orders of magnitude (1,000-fold greater). The large age dependence and large values of vDFR quantified in this study of 17 countries on 4 continents, using all the main COVID-19 vaccine types and manufacturers, should induce governments to immediately end the baseless public health policy of prioritizing elderly residents for injection with COVID-19 vaccines, until valid risk-benefit analyses are made.
32 -
Newname wrote:
Seventeen equatorial and Southern-Hemisphere countries were studied (Argentina, Australia, Bolivia, Brazil, Chile, Colombia, Ecuador, Malaysia, New Zealand, Paraguay, Peru, Philippines, Singapore, South Africa, Suriname, Thailand, Uruguay), which comprise 9.10 % of worldwide population, 10.3 % of worldwide COVID-19 injections (vaccination rate of 1.91 injections per person, all ages), virtually every COVID-19 vaccine type and manufacturer, and span 4 continents.
In the 17 countries, there is no evidence in all-cause mortality (ACM) by time data of any beneficial effect of COVID-19 vaccines. There is no association in time between COVID-19 vaccination and any proportionate reduction in ACM. The opposite occurs.
All 17 countries have transitions to regimes of high ACM, which occur when the COVID-19 vaccines are deployed and administered. Nine of the 17 countries have no detectable excess ACM in the period of approximately one year after a pandemic was declared on 11 March 2020 by the World Health Organization (WHO), until the vaccines are rolled out (Australia, Malaysia, New Zealand, Paraguay, Philippines, Singapore, Suriname, Thailand, Uruguay). Unprecedented peaks in ACM occur in the summer (January-February) of 2022 in the Southern Hemisphere, and in equatorial-latitude countries, which are synchronous with or immediately preceded by rapid COVID-19-vaccine-booster-dose rollouts (3rd or 4th doses). This phenomenon is present in every case with sufficient mortality data (15 countries).
Two of the countries studied have insufficient mortality data in January- February 2022 (Argentina and Suriname). Detailed mortality and vaccination data for Chile and Peru allow resolution by age and by dose number. It is unlikely that the observed peaks in all-cause mortality in January- February 2022 (and additionally in: July-August 2021, Chile; July-August 2022, Peru), in each of both countries and in each elderly age group, could be due to any cause other than the temporally associated rapid COVID-19-vaccine-booster-dose rollouts.
Likewise, it is unlikely that the transitions to regimes of high ACM, coincident with the rollout and sustained administration of COVID-19 vaccines, in all 17 Southern- Hemisphere and equatorial-latitude countries, could be due to any cause other than the vaccines. Synchronicity between the many peaks in ACM (in 17 countries, on 4 continents, in all elderly age groups, at different times) and associated rapid booster rollouts allows this firm conclusion regarding causality, and accurate quantification of COVID-19-vaccine toxicity. The all-ages vaccine-dose fatality rate (vDFR), which is the ratio of inferred vaccine- induced deaths to vaccine doses delivered in a population, is quantified for the January- February 2022 ACM peak to fall in the range 0.02 % (New Zealand) to 0.20 % (Uruguay). In Chile and Peru, the vDFR increases exponentially with age (doubling approximately every 4 years of age), and is largest for the latest booster doses, reaching approximately 5 % in the 90+ years age groups (1 death per 20 injections of dose 4). Comparable results occur for the Northern Hemisphere, as found in previous articles (India, Israel, USA). We quantify the overall all-ages vDFR for the 17 countries to be (0.126 ± 0.004) %, which would imply 17.0 ± 0.5 million COVID-19 vaccine deaths worldwide, from 13.50 billion injections up to 2 September 2023. This would correspond to a mass iatrogenic event that killed (0.213 ± 0.006) % of the world population (1 death per 470 living persons, in less than 3 years), and did not measurably prevent any deaths. The overall risk of death induced by injection with the COVID-19 vaccines in actual populations, inferred from excess all-cause mortality and its synchronicity with rollouts, is globally pervasive and much larger than reported in clinical trials, adverse effect monitoring, and cause-of-death statistics from death certificates, by 3 orders of magnitude (1,000-fold greater). The large age dependence and large values of vDFR quantified in this study of 17 countries on 4 continents, using all the main COVID-19 vaccine types and manufacturers, should induce governments to immediately end the baseless public health policy of prioritizing elderly residents for injection with COVID-19 vaccines, until valid risk-benefit analyses are made.
The Unkle has learned to copy-paste! No more links to bitchut videos!
34 -
2600 bro wrote:
Youve convinced me
1359 days since the Covid madness started.
1080 days of "vaccine" availability.
Unvaxxed through the 1080 days.
Sick 2 days out of the 1359 days.
Still waiting for horrible things to happen.
I pity the poor vax crazy zealots.
44 -
DanM wrote:
2600 bro wrote:
Youve convinced me
1359 days since the Covid madness started.
1080 days of "vaccine" availability.
Unvaxxed through the 1080 days.
Sick 2 days out of the 1359 days.
Still waiting for horrible things to happen.
I pity the poor vax crazy zealots.
Do you know the vaccine status of Munger and Kissinger? Why is nobody asking these questions?
31 -
Do you realize that they were 99 and 100 years old ?!?
01 -
Slower at 86 wrote:
Do you realize that they were 99 and 100 years old ?!?
Probably added to the official count of Covid deaths
13 -
Harambe wrote:
The Unkle has learned to copy-paste! No more links to bitchut videos!
It's more Dennis Rancourt linked and extensively debunked here:
What I find interesting about this sort of misinformation is that a significant amount of work was put into this paper by persons with apparently reasonable levels of analytic skill who surely must be aware of the obvious flaws of the paper, yet they repeat them over and over.
They are clearly malicious actors preying on a gullible subset of the population.23 -
Harambe wrote:
Do you know the vaccine status of Munger and Kissinger? Why is nobody asking these questions?
A more useful approach is to examine the fate of lesser known people. I posted the story of one woman, Diane Clehane. She was 61.
03 -
DanM wrote:
Harambe wrote:
Do you know the vaccine status of Munger and Kissinger? Why is nobody asking these questions?
A more useful approach is to examine the fate of lesser known people. I posted the story of one woman, Diane Clehane. She was 61.
Sources say Kissinger was multi-jabbed. This is a bombshell.
15