Monkeys typing wrote:
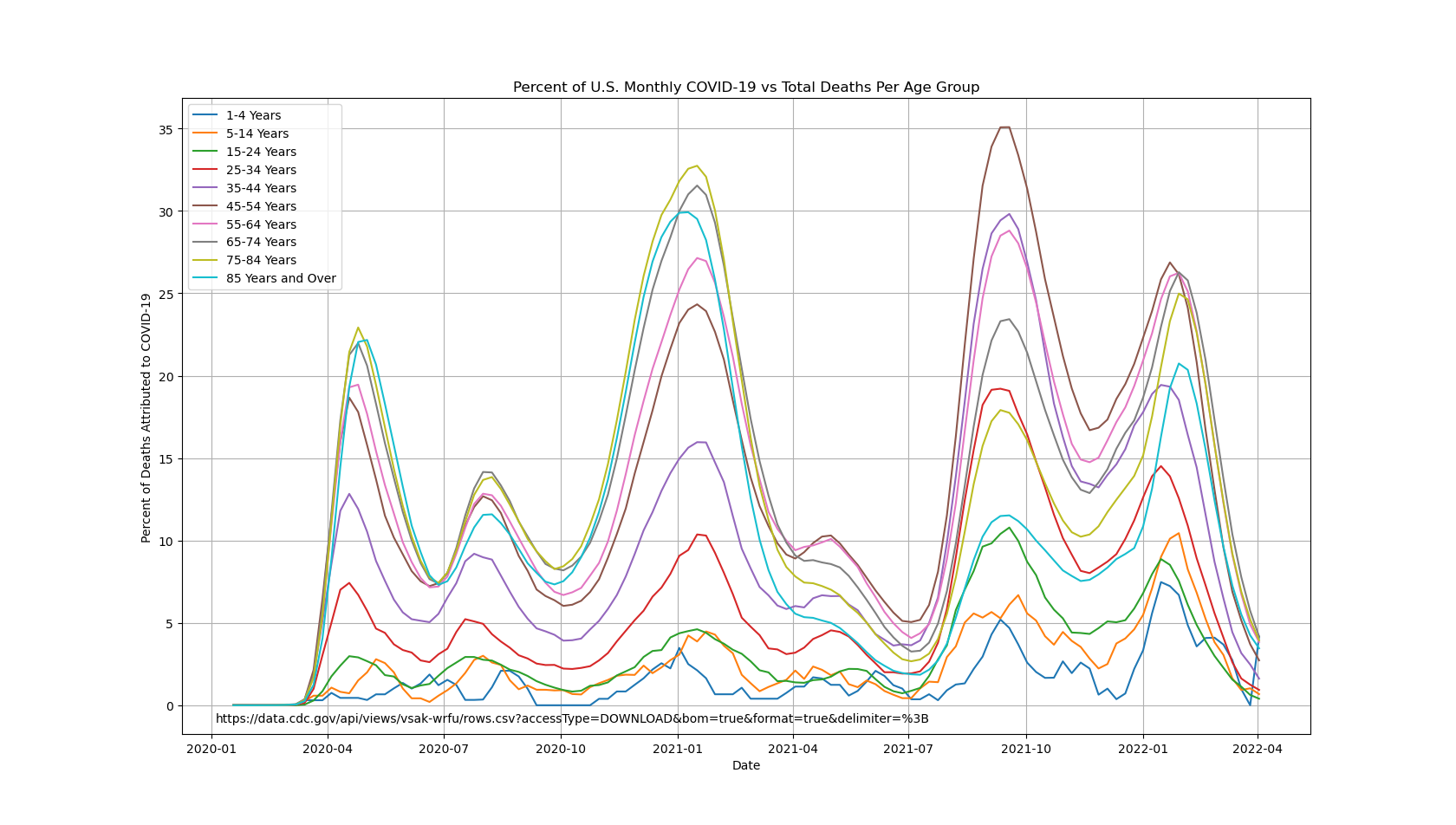
It's smaller than older age groups for 0-44, but "almost no impact" is misleading.
https://monkeystyping.neocities.org/PercentOfUSWeeklyCovidDeathsByAge.png
{kind=link}
Almost no impact sounds about right.
Monkeys typing wrote:
It's smaller than older age groups for 0-44, but "almost no impact" is misleading.
https://monkeystyping.neocities.org/PercentOfUSWeeklyCovidDeathsByAge.png
Almost no impact sounds about right.
The childhood diseases are so as a consequence of high contagion and lifetime immunity, with approximate relation
R0 = 1+ L/A
where L is life expectancy and A is average age of disease onset. Result of Klaus Dietz as reported by Anderson and May, Directly transmitted infectious diseases: control by vaccination, in Science, new series 1982, Vol. 215, 1053-1060.
SARS COV 2 will probably be one of many seasonal colds, but never again so prevalent. The susceptible fraction of the population will be smaller than this past year. It may have a quasi-cyclic behavior as population immunity naturally waxes and wanes. These patterns are described by Anderson and May in the work cited and other work from about the same time.
For those at heightened risk of a bad COVID-19 outcome, vaccination seems a prudent choice. For those at low risk, maybe not so much, and maybe that calculation changes as we get years of experience with the vaccine.
If our elites really cared about people living better, they could have used this past year to hammer home the importance of conquering diet and lifestyle induced obesity. Instead, our elites encouraged the opposite.
pinesol wrote:
If our elites really cared about people living better, they could have used this past year to hammer home the importance of conquering diet and lifestyle induced obesity. Instead, our elites encouraged the opposite.
Modern Politics 101: Never let yourself be accused of blaming the victim, even if they deserve it.
Doctors counseling patients about weight seems to have mixed results, so I’m not sure reminding them of their weight status will get you where you want to do. An extremely effective tobacco prevention intervention is the tobacco tax. From the WHO article below. “
Several reviews have demonstrated that a price increase of 10% results in a decrease of 2.5% to 5% in cigarette consumption”
One could imagine taxing sweeteners and funding vegetable affordability/accessibility projects
I doubt that is politically feasible
As mentioned in previous threads, when Michelle Obama addressed the issue it was not received well.
I would have wanted more people getting exercise in the woods (not MY woods, of course), and while that my not be accessible to the inner city poor, it definitely can be to the old mill city poor. Unfortunately, for at least some of these folks, it is so foreign as to be frightening.
There are several far more accurate ways to estimate how many have been infected.
1. The death rate generally is 1 in 200. COVID related deaths aren't being missed in any significant number. Nor are they being overestimated. They match up well with all cause mortality numbers. So multiply deaths by 200 and that will give you a rough estimate of total infected as of 2 to 3 weeks ago...as deaths are delayed by that much. This puts us at 80 million infected, presumably immune. This is roughly 25% of the US population. A big chunk, but not enough for herd immunity.
2. Antibody studies. This is a very accurate way of estimating how many have been infected in total. Unfortunately there haven't been many formal studies done lately on this, but state data is widely available. They indicate somewhere between 20 and 30% have been infected depending on where you live.
We are far from "herd immunity". But the worst will be behind us by March. Especially with vaccines ramping up. It might slow a bit with a big chunk immune so far, but we've still got a few months of real bad pain left.
joedirtty wrote:
The best estimate of IFR that I have seen is 0.26% and most behavior I have seen tends to follow that threshold. Using that figure would put us at about 148,000,000 cases, which is fairly close to the number you have posited, which puts us at about a 45-50% exposure rate. Now that they are starting to vaccinate the 70+ crowd (who account for about 80% of COVID deaths), we should start to see a significant decline in deaths in a month or two. There are a number of cities and counties in the US that are already pretty much at herd immunity.
Take for example NYC, that has only seen an approximate 8% increase in its deaths since November (as opposed to many cities that have seen their death total double or more over that same time interval). Pull up NYC under the jurisdiction on the CDC excess deaths website and you will visually be able to see this in play:
https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htmFor the first time in the pandemic New York actually said something that made sense in that they could no longer afford to keep the economy locked down (and quite honestly, they should have opened it completely since the summer, but they decided to ignore the science and follow the fear:
https://www.foxnews.com/politics/critics-mock-gov-cuomo-for-sudden-denunciation-of-lockdowns-suggest-trump-is-using-his-twitter-account
An IFR of 1 in 400 would massively overestimate that number infected. This would but us at 50% of the population infected so far nationwide. This is not supported by anything in the antibody studies or by common sense. No way we're anywhere near 50%.
A simple calculation of NY or NJ shows the massive flaws here. NY for example: 40,000+ deaths X 400 = over 16 MILLION infected out of 19 million. Absolutely no way 85% of NY has been infected.
runnER/DR wrote:
There are several far more accurate ways to estimate how many have been infected.
1. The death rate generally is 1 in 200. COVID related deaths aren't being missed in any significant number. Nor are they being overestimated. They match up well with all cause mortality numbers. So multiply deaths by 200 and that will give you a rough estimate of total infected as of 2 to 3 weeks ago...as deaths are delayed by that much. This puts us at 80 million infected, presumably immune. This is roughly 25% of the US population. A big chunk, but not enough for herd immunity.
2. Antibody studies. This is a very accurate way of estimating how many have been infected in total. Unfortunately there haven't been many formal studies done lately on this, but state data is widely available. They indicate somewhere between 20 and 30% have been infected depending on where you live.
We are far from "herd immunity". But the worst will be behind us by March. Especially with vaccines ramping up. It might slow a bit with a big chunk immune so far, but we've still got a few months of real bad pain left.
Your numbers are probably correct for the US.
There are diffences between countries.
FHI (the CDC of Norway) estimated in late november that 100 000 had been infected based on antibody studies.
At the time, less than 400 had died (The total number of dead from Covid passed 500 today) which implies an IFR of +/- 0,40%.
That includes spring wave where prognosis was worse, so a reasonable estimate for Norway would actually be that current IFR is probably 0,35% max..
My guess is that demographic plays a role (Less obesity and less people of color in Norway compared to US).
Level of health care too of course, but that's probably not a big factor when comparing
Even CFR rate in Norway is under 0,9%... (509 dead, 57282 infected as per today).
runnER/DR wrote:
joedirtty wrote:
The best estimate of IFR that I have seen is 0.26% and most behavior I have seen tends to follow that threshold. Using that figure would put us at about 148,000,000 cases, which is fairly close to the number you have posited, which puts us at about a 45-50% exposure rate. Now that they are starting to vaccinate the 70+ crowd (who account for about 80% of COVID deaths), we should start to see a significant decline in deaths in a month or two. There are a number of cities and counties in the US that are already pretty much at herd immunity.
Take for example NYC, that has only seen an approximate 8% increase in its deaths since November (as opposed to many cities that have seen their death total double or more over that same time interval). Pull up NYC under the jurisdiction on the CDC excess deaths website and you will visually be able to see this in play:
https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htmFor the first time in the pandemic New York actually said something that made sense in that they could no longer afford to keep the economy locked down (and quite honestly, they should have opened it completely since the summer, but they decided to ignore the science and follow the fear:
https://www.foxnews.com/politics/critics-mock-gov-cuomo-for-sudden-denunciation-of-lockdowns-suggest-trump-is-using-his-twitter-accountAn IFR of 1 in 400 would massively overestimate that number infected. This would but us at 50% of the population infected so far nationwide. This is not supported by anything in the antibody studies or by common sense. No way we're anywhere near 50%.
A simple calculation of NY or NJ shows the massive flaws here. NY for example: 40,000+ deaths X 400 = over 16 MILLION infected out of 19 million. Absolutely no way 85% of NY has been infected.
I agree with your general point (absolutely no way that 85% of New York have been infected, but that calculation discounts that prognosis was much worse in march/april than now, and the bulk of people that succumed to Covid in those states did so in that early period.
Even adjusting for that, lets say IFR was 0,67% (for simplicity, quite plausably it was even higher in the spring) in NY/ in spring, the number would be 12 million or close to 65% which still sounds way too high.
I guess what I am trying to say is that one should be careful using current IFR when projecting number of infected for the entire pandemic, as that would typically lead to overestimating number of infected in areas where significant portion of deaths occured in first wave.
I am not going to pretend to know more than you on prognosis on Covid of course, but I remember the IFR was typically estimated to be over 1% in march, 0,5-1% by summer and have been adjusted downwards since as treatment have become better.
By the way, I am also not claiming CURRENT IFR is as low as 0,25%, but probably lower than 0,5% quite a few places.
devil's advocate wrote:
...unless immunity is short-lived.
Its not really even immunity. Its minimizing the outcome.
All a vaccine does is prepare your body to fight the virus off.
You can still get it and spread it, but you'll be more like an asymptomatic patient.
Its why as soon as we get a large number of people vaxxed up, the confidence will rise and the death rate will go up for a period as the antivaxxers high five themselves
There's basically no model where a vaccine does not decrease transmission significantly. Viral load and transmissibility are highly correlated and vaccines universally reduce viral load.
miomago wrote:
devil's advocate wrote:
...unless immunity is short-lived.
Its not really even immunity. Its minimizing the outcome.
All a vaccine does is prepare your body to fight the virus off.
You can still get it and spread it, but you'll be more like an asymptomatic patient.
Its why as soon as we get a large number of people vaxxed up, the confidence will rise and the death rate will go up for a period as the antivaxxers high five themselves
2600 bro, you are correct, the support for significant asymptomatic spread from vaccinated people has been decimated.
I was arguing the side “we don’t know if it will prevent transmission” but separate info on the moderna and Pfizer vaccine has come in recently showing extremely encouraging data about a high degree of transmission prevention.
trashcan wrote:
2600 bro, you are correct, the support for significant asymptomatic spread from vaccinated people has been decimated.
I was arguing the side “we don’t know if it will prevent transmission” but separate info on the moderna and Pfizer vaccine has come in recently showing extremely encouraging data about a high degree of transmission prevention.
Care to expand on that? I’ve been expecting this but haven’t seen much published.
joedirtty wrote:
Monkeys typing wrote:
Source?
Source:
https://www.nber.org/papers/w28303
Your source doesn’t support your claim.
pinesol wrote:
The childhood diseases are so as a consequence of high contagion and lifetime immunity, with approximate relation
R0 = 1+ L/A
where L is life expectancy and A is average age of disease onset. Result of Klaus Dietz as reported by Anderson and May, Directly transmitted infectious diseases: control by vaccination, in Science, new series 1982, Vol. 215, 1053-1060.
SARS COV 2 will probably be one of many seasonal colds, but never again so prevalent. The susceptible fraction of the population will be smaller than this past year. It may have a quasi-cyclic behavior as population immunity naturally waxes and wanes. These patterns are described by Anderson and May in the work cited and other work from about the same time.
For those at heightened risk of a bad COVID-19 outcome, vaccination seems a prudent choice. For those at low risk, maybe not so much, and maybe that calculation changes as we get years of experience with the vaccine.
If our elites really cared about people living better, they could have used this past year to hammer home the importance of conquering diet and lifestyle induced obesity. Instead, our elites encouraged the opposite.
This is the best Covid post of the year
mein unkle wrote:
joedirtty wrote:
Source:
https://www.nber.org/papers/w28303Your source doesn’t support your claim.
I'll help you with math. At the time the paper was written, there were 250,000 excess deaths. Approximately 30,000 of these were non-covid excess deaths of despair and they were estimating there was an additional under count of 17,000 covid deaths. So, of the 267,000 excess deaths over this period, approximately 30,000 of these are non-covid excess deaths of despair. 30 / 267 = 11.23%, which is a little over 10%.
I don't need to know math well if I know there's 4000 a day dying from it and thinking about the not so distance future whether that's 1 week or 6 months. You know as in multiplying with 7 or 180 or whatever.
What’s going to run out of gas sooner, Covid or Trump conspiracy theories?
It's quite obvious that they're trying to manufacture a peak in coronavirus around Jan 20th to give the illusion of Biden causing a descent
jamin wrote:
It's quite obvious that they're trying to manufacture a peak in coronavirus around Jan 20th to give the illusion of Biden causing a descent
Ok, so Covid it is
RIP: D3 All-American Frank Csorba - who ran 13:56 in March - dead
RENATO can you talk about the preparation of Emile Cairess 2:06
Running for Bowerman Track Club used to be cool now its embarrassing
Hats off to my dad. He just ran a 1:42 Half Marathon and turns 75 in 2 months!
Great interview with Steve Cram - says Jakob has no chance of WRs this year
Rest in Peace Adrian Lehmann - 2:11 Swiss marathoner. Dies of heart attack.